Cms L564 Printable Form
Cms L564 Printable Form - If you are applying during the special enrollment period, also fill out the request for employment information. Fill out the request for employment information online and print it out for free. Then you send both together to your local social security. Learn what you need to complete the. This form is used for proof of group health care coverage based on current employment. This information is needed to process your medicare enrollment application. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more. To be completed by individual signing up for medicare part b (medical insurance) Request for employment information section a: Then, submit the form to your employer for them to complete. Request for employment information section a: Provide relevant details about your employer and your employment. Then you send both together to your local social security. This information is needed to process your medicare enrollment application. This form is used for proof of group health care coverage based on current employment. Fill out the request for employment information online and print it out for free. Learn what you need to complete the. Then, submit the form to your employer for them to complete. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more. If you are applying during the special enrollment period, also fill out the request for employment information. Provide relevant details about your employer and your employment. This information is needed to process your medicare enrollment application. Fill out the request for employment information online and print it out for free. This form is used for proof of group health care coverage based on current employment. Then, submit the form to your employer for them to complete. Provide relevant details about your employer and your employment. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more. This information is needed to process your medicare enrollment application. This form is used for proof of group health. Provide relevant details about your employer and your employment. Learn what you need to complete the. If you are applying during the special enrollment period, also fill out the request for employment information. To be completed by individual signing up for medicare part b (medical insurance) This form is used for proof of group health care coverage based on current. Then, submit the form to your employer for them to complete. To be completed by individual signing up for medicare part b (medical insurance) Request for employment information section a: Then you send both together to your local social security. Fill out the request for employment information online and print it out for free. If you are applying during the special enrollment period, also fill out the request for employment information. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more. Then, submit the form to your employer for them to complete.. This form is used for proof of group health care coverage based on current employment. Then you send both together to your local social security. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more. Learn what you. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more. Request for employment information section a: Provide relevant details about your employer and your employment. To be completed by individual signing up for medicare part b (medical insurance). Request for employment information section a: Then, submit the form to your employer for them to complete. Learn what you need to complete the. This information is needed to process your medicare enrollment application. Then you send both together to your local social security. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more. To be completed by individual signing up for medicare part b (medical insurance) If you are applying during the special enrollment period, also fill out the request for. Provide relevant details about your employer and your employment. Then you send both together to your local social security. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more. This information is needed to process your medicare enrollment. This form is used for proof of group health care coverage based on current employment. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more. Learn what you need to complete the. If you are applying during the special enrollment period, also fill out the request for employment information. Fill out the request for employment information online and print it out for free. This information is needed to process your medicare enrollment application. Then you send both together to your local social security. Provide relevant details about your employer and your employment.
Cms L564 Printable Form Printable Forms Free Online

Printable Form Cms L564 Fillable Form 2022

Form CMSL564
Cms L564 Form Printable Printable Forms Free Online

Form Cms L564 Printable Printable Forms Free Online

The Medicare Form CMSL564 for Employers
Cms L564 Printable Form

Form CMS L564 / R297 template ONLYOFFICE

Fillable Online Request for CMSL564 Form Fax Email Print pdfFiller

Cms L564 Printable Form
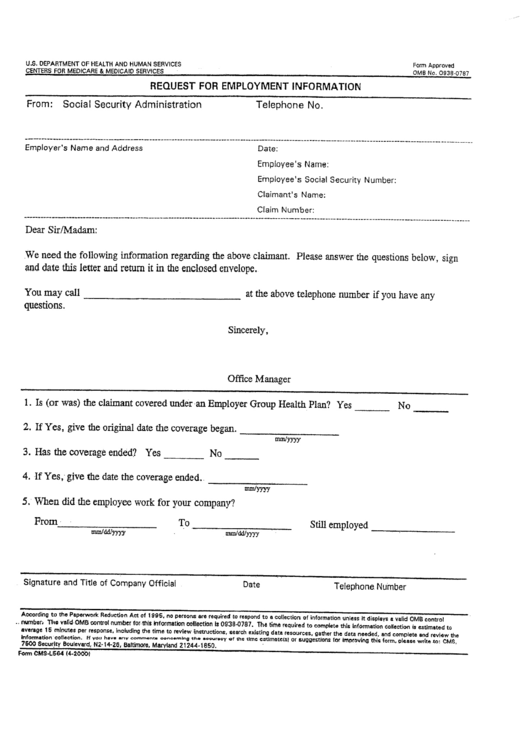
Then, Submit The Form To Your Employer For Them To Complete.
Request For Employment Information Section A:
To Be Completed By Individual Signing Up For Medicare Part B (Medical Insurance)
Related Post: